

ADVERTISEMENT
Total Contact Cast Use in Patients With Peripheral Arterial Disease: A Case Series and Systematic Review
Abstract
Introduction. As the majority of diabetic foot ulcerations (DFUs) occur on the plantar foot, excessive pressure is a major contributing factor to delayed healing. The gold standard for offloading is the total contact cast (TCC); yet, TCC use is contraindicated in patients with ischemia. Lower extremity ischemia typically presents in the more severe end stages of peripheral arterial disease (PAD). As PAD exists on a severity spectrum from mild to severe, designation of a clear cutoff where TCC use is an absolute contraindication would assist those who treat DFUs on a daily basis. Objective. The aim of this study is to determine if a potential cutoff value for PAD where TCC use would be an absolute contraindication could be ascertained from a retrospective case series and a systematic literature review of patients with PAD in which treatment included TCC use. Materials and Methods. A retrospective cases series and systematic review of patients with mild to moderate PAD treated with a TCC was performed. All reports of TCC use in patients with PAD and a neuropathic ulceration that included results of noninvasive vascular studies were included. Results. Results suggested that TCC use is a viable treatment modality for pressure-related DFUs in patients with an ankle pressure ≥ 80 mm Hg, a toe pressure ≥ 74 mm Hg, an ankle-brachial index ≥ 0.55, or a toe-brachial index ≥ 0.55. Conclusions. Vascular evaluation, individual risk/benefit analysis, close follow-up, and patient education are essential components of TCC use in these patients. Repeat vascular evaluation is recommended if the wound fails to progress towards resolution with TCC use.
Introduction
The prevalence of peripheral arterial disease (PAD) in the general population ranges from 10% to 40%.1,2 In the clinical practice guidelines for management of the diabetic foot put forth by the Society for Vascular Surgery, the American Podiatric Medical Association, and the Society for Vascular Medicine, at least 65% of diabetic foot ulcerations (DFUs) are reported to be complicated by PAD.1 The Eurodiale study, a 1-year retrospective review of all patients presenting with a DFU at 14 diabetic foot centers in Europe, found that 61% of patients had PAD.2 Of these patients, 49% were defined as having moderate PAD, with an ankle-brachial index (ABI) < 0.9 or absent palpable pedal pulses, and 12% were defined as having severe PAD with an ABI < 0.5. In addition, 32% of patients had falsely elevated ABIs, making the diagnosis of PAD severity difficult. The prevalence of PAD was found to increase with age > 70 years and the presence of disabling comorbidities. Healing rates were worst when DFUs were complicated by both PAD and infection. However, these types of ulcerations occurred more often on the dorsal aspect of the foot where pressure is less likely to be a contributing factor to delayed healing.2
Offloading has been reported to be the single most important factor in the resolution of plantar neuropathic ulcerations.3,4 Postoperative shoe and removable cast walker use are the most common offloading modalities employed.5-8 However, these offloading modalities rely heavily on patient compliance with use for success. Studies have shown that patients often only use these devices between 2% to 28% of waking/walking hours, making the associated prolonged healing times and greater incidence of infection and amputation not surprising.9-11 Dr. Paul Brand brought the concept of the total contact cast (TCC) to the United States in the 1960s as a treatment for leprosy-related neuropathic ulcerations.12 The TCC later became touted as the gold standard for offloading plantar DFUs as it forces patient compliance; provides the greatest reduction in peak plantar pressures, particularly to the forefoot; and has reported resolution rates ≥ 73%.3,5,6,8,10,13-21 However, its use remains limited due to a variety of clinician, organization, and patient-related barriers. One of these barriers is the contraindication of use when ischemia or severe PAD is present, although a clear definition or cutoff value has not been defined.5,8,21-29
As PAD exists on a spectrum of severity, with ischemia typically noted in the end stages, and the prevalence of neuroischemic neuropathic ulcerations on the rise, a clear cutoff value for PAD that would make TCC use an absolute contraindication would assist clinical decision-making for these patients. The aim of this study is to determine if a potential cutoff value for PAD where TCC use would be an absolute contraindication could be ascertained from a retrospective case series and a systematic literature review of patients with PAD in which treatment included TCC use.
Materials and Methods
A retrospective case series and a systematic review of patients with PAD and a plantar neuropathic ulceration that was treated with a TCC was performed. The retrospective cases came from 2 clinics that specialized in the treatment of chronic wounds. All selected cases involved the use of a TCC in patients with a diagnosis of PAD.
Literature search was restricted to English language, peer-reviewed journals, and utilized an inclusive text word query of ischemia OR peripheral arterial disease OR arterial insufficiency AND total contact cast AND neuropathic AND ulceration (with all-capital words representing the Boolean operators used). Literature search was performed from date of inception through December 2015. Each reference was then manually searched for additional pertinent references. All reports of TCC use in patients with PAD and a neuropathic ulceration that included results of noninvasive vascular studies were included. After identification and review of the included reports, data extracted from the studies included total number of patients, total number of feet, gender, laterality, patient age, duration of diabetes, duration of ulceration, vascular examination and noninvasive vascular study results, time to healing, unresolved wounds, amputation, and complications. The data collected were reviewed and analyzed in order to determine if a cutoff value for PAD where TCC use would be an absolute contraindication could be determined.
Results
Retrospective review
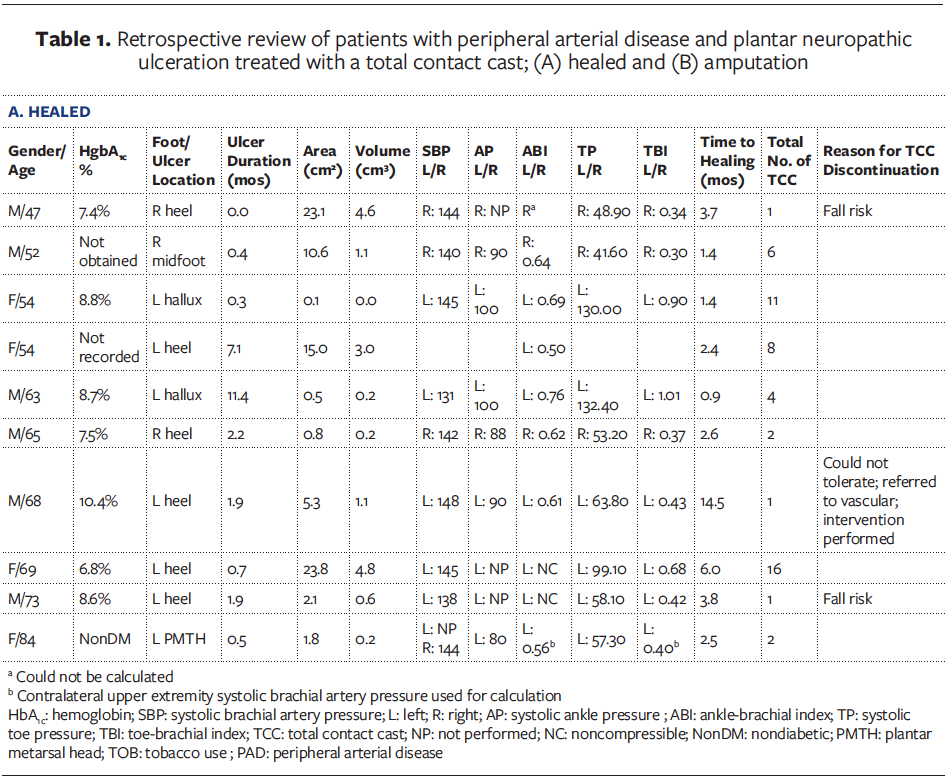
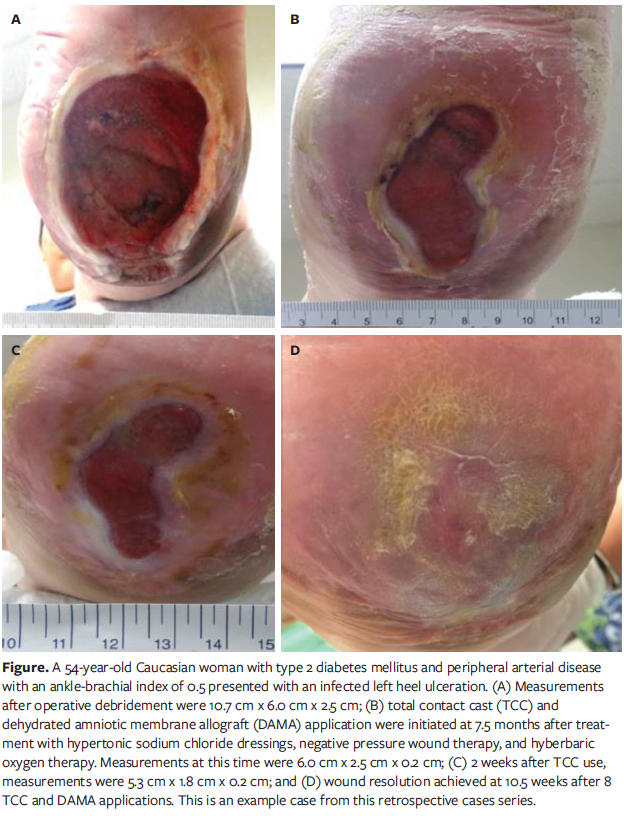
A total of 14 patients (10 males, 4 females) were identified (Table 1 and continued). The right foot was affected in 6 patients and the left in 8. Mean patient age was 61.5 ± 10.3 years (range, 47–84 years). Only 1 (7.1%) patient did not have diabetes mellitus. Hemoglobin A1c was recorded in 10 of the 13 remaining patients with a mean of 8.4% ± 1.5% (range, 6.2%–11.0%). The majority of ulcerations were located on the heel (7; 50%) followed by the metatarsal head (3; 21.4%), the hallux (3; 21.4%), and the midfoot (1; 7.1%). Mean ulcer duration was 1.9 ± 6.5 months (range, 0–24 months). Mean ulcer area was 2.1 ± 8.1 cm2 (range, 0–24 cm2). Mean ulcer volume was 0.5 ± 1.6 cm³ (range, 0–5 cm3) (Figure).
Systolic brachial artery pressure was obtained in the ipsilateral upper extremity for 13 patients and the contralateral upper extremity for 1 patient. Mean systolic brachial artery pressure on the left was 141.5 ± 11.7 mm Hg (range, 117–148 mm Hg) and 142.0 ± 25.9 mm Hg (range, 99–183 mm Hg) on the right. Mean systolic ankle pressure for the left and right lower extremities were similar at 90.0 ± 11.7 mm Hg (range, 70–140 mm Hg) and 90.0 ± 26.7 mm Hg (range, 70–140 mm Hg), respectively. Mean ABI for the left and right lower extremities also were similar at 0.62 ± 0.9 mm Hg (range, 0.50–0.76 mm Hg) and 0.62 ± 0.36 mm Hg (range, 0.59–1.41 mm Hg), respectively. Mean systolic toe pressure and toe-brachial index (TBI) did vary from left to right: 94.4 ± 32.3 mm Hg (range, 57.3–132.4 mm Hg) and 53.2 ± 21.0 mm Hg (range, 41.6–95.0 mm Hg) compared with 0.68 ± 0.25 mm Hg (range, 0.40–1.01 mm Hg) and 0.37 ± 0.27 mm Hg (range, 0.30–0.96 mm Hg), respectively.
Ten (71.4%) patients achieved wound resolution. Mean time to healing was 2.5 ± 4.2 months (range, 0–14.5 months). An average of 5.2 ± 5.1 (range, 1–16) TCC applications were performed. Only 1 (10%) patient could not tolerate the TCC after 1 application. This patient was referred for vascular evaluation and underwent revascularization, which resulted in wound resolution 1.3 months later. Discontinuation of TCC occurred in 2 other patients as they were deemed to be a fall risk with the cast on. The remaining 7 (70%) patients continued with TCC use until deemed no longer necessary by the treating provider. Time to healing differed between the 7 patients who continued TCC use compared with the 3 who discontinued TCC use after 1 application, 3.7 ± 4.2 months versus 7.3 ± 6.2 months, respectively.
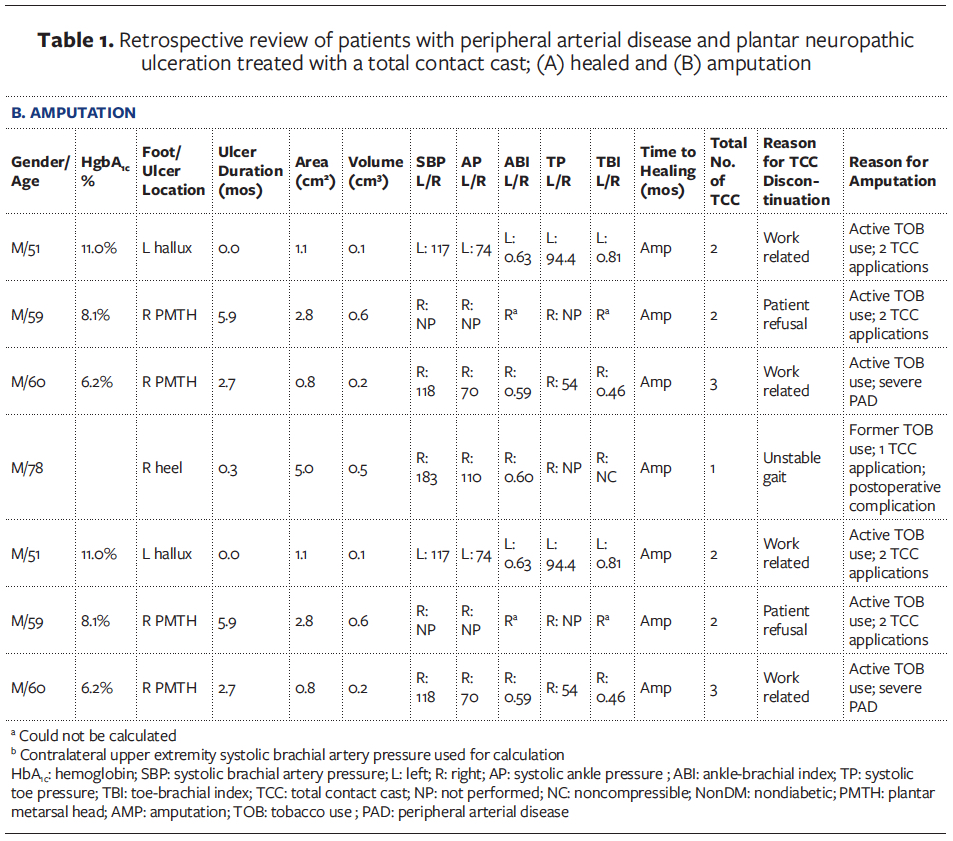
Four (28.6%) patients underwent amputation. None of the amputations occurred from complications sustained from TCC application technique or use. A similar factor for each of these patients was discontinuation of TCC use: work related (2 patients), unstable gait (1 patient), and refusal with continuation of use (1 patient). Average TCC applications were 2.0 ± 0.8 (range, 1–3). The 2 patients who discontinued TCC use for work-related reasons were both active tobacco users; 1 had a plantar metatarsal head ulceration and history of severe PAD with prior revascularization performed and no options for further intervention. The other patient had a hallux amputation. Upon discontinuation of TCC use in both of these patients, their wounds subsequently worsened and necessitated partial foot amputation. The remaining 2 patients (unstable gait and refusal to use) both had a below-knee amputation. One had a recurrent plantar metatarsal head ulceration that had previously healed in 1 month with 6 TCC applications; this patient refused continued TCC use and underwent amputation 5 months later. The second patient had ulceration of the heel; a rotational flap was attempted for closure and failed in the immediate postoperative period due to the patient stepping on the foot.
Systematic review
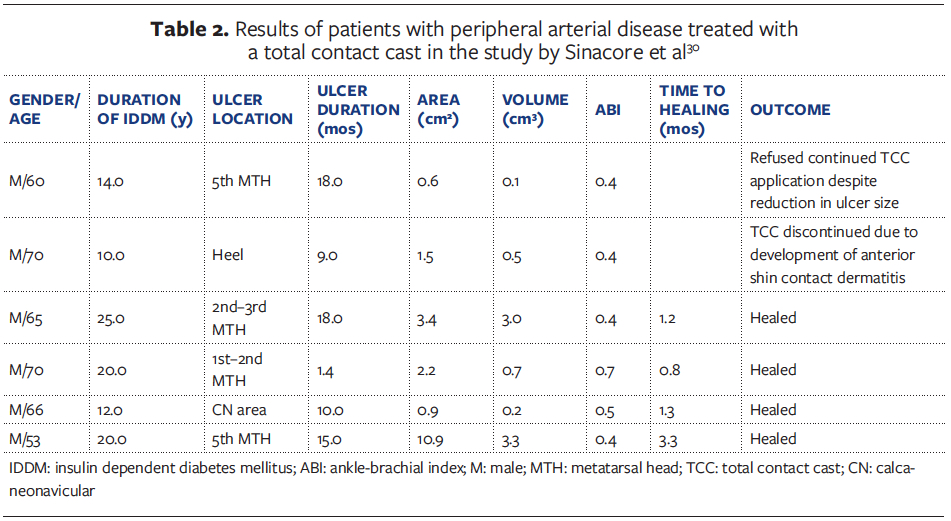
The literary search for potentially eligible information yielded a total of 8 references of which only 1 (12.5%) contained patient-specific, noninvasive vascular study results.30 Level of evidence for this study was Level 4, therapeutic, and the methodological quality was fair. Results of 6 patients were reported. Mean patient age was 65.5 ± 6.5 years (range, 53–70 years). Mean diabetes duration was 17.0 ± 5.7 years (range, 10–25 years). Mean ulcer duration was 12.5 ± 6.4 months (range, 1.4–18 months). Mean ulcer area and volume were 1.9 ± 3.9 cm2 (range, 0.6–10.9 cm2) and 0.6 ± 1.5 cm3 (range, 0.1–3.0 cm3), respectively. The mean ABI was 0.4 ± 0.1 (range, 0.4–0.7). Four (66.7%) patients healed at a mean of 1.3 ± 1.1 months (range, 0.8–3.3 months). The remaining 2 patients had unresolved ulcerations, although 1 of these patients with a heel ulceration had TCC treatment discontinued after development of anterior shin contact dermatitis, and the other refused additional TCC applications despite reduction in size of their plantar fifth metatarsal head ulceration (Table 230).
Discussion
Total contact cast use is currently contraindicated in the presence of PAD and/or ischemia. However, a clear cutoff value has never been defined. It is the responsibility of the provider to weigh the risks and benefits of TCC use for each patient with PAD to determine if a trial of use is indicated as treatment for a pressure- related neuropathic ulceration. This retrospective case review and additional systematic literature review provides evidence that TCC use in patients with an ankle pressure ≥ 90 mm Hg, a toe pressure ≥ 74 mm Hg, an ABI ≥ 0.5, or a TBI ≥ 0.5 may be a viable option for treatment of pressure-related DFUs. While only 1 study30 provided specific data on TCC use in patients with PAD, several studies12,27,31-37 did include patients with PAD and a DFU who were treated with a TCC. Results gleaned from these articles combined with the results herein suggest that TCC use may be a treatment option in patients with an ankle pressure ≥ 80 mm Hg, a toe pressure ≥ 74 mm Hg, an ABI ≥ 0.55, or a TBI ≥ 0.55 and a pressure-related neuropathic ulceration.12,27,30-37
One retrospective review,35 which did not include results of noninvasive vascular studies, reported a 100% resolution rate (6 patients, 8 ulcerations) in a mean of 5 weeks. Wound resolution occurred for the oldest patient in the study (aged 75 years) despite the patient having a nonpalpable dorsalis pedis artery.35
A retrospective review30 of 30 patients (33 DFUs) treated with a TCC included the treatment of 6 patients with PAD (defined as having an ABI < 1.0). All 6 patients were male, had insulin-dependent diabetes mellitus for an average of 16.8 ± 5.7 years (range, 53–70 years), and had an average ABI of 0.5 ± 0.1 (range, 0.38–0.66) (Table 230). Average ulceration duration was 11.9 ± 6.4 months (range, 1.4–18 months). Average ulcer area and volume was 3.3 ± 3.9 cm2 (range, 0.61–0.9 cm2) and 1.3 ± 1.5 cm3 (range, 0.1–3.3 cm3), respectively. Of the 6 patients, 4 (66.7%) achieved wound resolution at an average of 1.6 ± 1.1 months (range, 0.8–3.3 months). Of the 2 unresolved wounds, 1 was a heel ulceration where TCC use was discontinued after the patient developed contact dermatitis on the anterior shin and the other was a plantar fifth metatarsal head ulceration that had reduced in size prior to patient refusal of continued TCC application.30
Two retrospective reviews included patients with an ABI ≥ 0.45 and a systolic ankle pressure ≥ 70 mm Hg.33,34 A 73% healing rate in just over 1 month was reported in the study by Helm et al.33 The other study by Walker et al34 developed a predictive equation for the healing time of both forefoot and nonforefoot ulcerations treated with a TCC via regression analysis. These predictive equations were based on patient age and gender and ulcer duration, grade, and long and short diameters; PAD was not found to be a contributing factor.34 Laing et al12 performed a retrospective review on 46 patients (36 diabetics, 10 nondiabetics) with 56 plantar neuropathic ulcerations. Ulcerations were present for a mean of 17 months. An 81% resolution rate at an average of 6 weeks was reported. Of the 8 unresolved ulcerations, 6 (75%) occurred in patients with an average ABI of 0.61 (range, 0.44–0.81). One of these unresolved ulcerations (plantar fifth metatarsal head) lead to partial fifth ray resection due to the patient waiting 1 week to be seen despite experiencing pain beginning 2 days after TCC application (ABI = 0.67). Given the results of their respective studies, all authors12,30,33-35 found that a trial of TCC use in patients with a pressure-related ulceration and PAD, defined as an ABI > 0.44 and < 1.0, was reasonable as wounds only failed to progress and did not worsen if patients were seen promptly. Individual patient risk and benefit assessment and the importance of patient education were stressed. Vascular evaluation was recommended if these wounds failed to progress after initiation of TCC use.12,30,33,34 It must be stated that all of these studies occurred in the late 1980s and 1990s. Expeditious vascular evaluation is currently recommended for any patient where a concern of PAD exists.
Three studies26,36,37 involved the prospective collection of data on TCC use for the treatment of DFUs. Mueller et al36 performed a prospective, controlled clinical trial comparing TCC use with daily dressing changes. No significant difference existed between the 2 study groups in regard to age, type of diabetes, duration of diabetes, ulcer duration, ulcer size, ulcer grade, severity of peripheral neuropathy, or presence of PAD (defined as an ABI > 0.5 and < 0.99). Two patients in the TCC group and 3 in the daily dressing change group had PAD, including 1 patient in each group who had an ABI < 0.5. A 90% resolution rate at a mean of 1.4 months was reported for the TCC group compared with a 32% resolution rate at a mean of 2.2 months for the daily dressing change group. Failure to achieve wound resolution was attributed to PAD for only 1 patient in the TCC group. While the patient achieved reduction in wound size during the 3-month study period, the ulceration remained unresolved. The patient developed a severe infection requiring hospitalization within 3 weeks of study completion and TCC discontinuation. The patient’s ABI at that time was 0.42 and was subsequently referred for formal vascular evaluation. No further follow-up was reported. Nabuurs-Franssen et al28 performed a 5-year retrospective review of prospectively collected data on TCC use in all patients within their facility who presented with a DFU. Of the 98 patients, 44% had PAD defined as no signs of critical limb ischemia (CLI) and 1 or more of the following: absent palpable pedal pulses, presence of intermittent claudication, an ABI < 0.9, a TBI < 0.6, and a transcutaneous oxygen pressure measurement (TCOM) between 30 mm Hg and 60 mm Hg. An overall healing rate of 76% at a mean of 33 days was reported. In patients with a noninfected DFU and PAD, a 69% healing rate at a mean of 42 days was reported. The presence of PAD did not hinder healing of any plantar first metatarsal head ulcerations or contribute to the development of superficial iatrogenic ulceration.
Ha Van et al37 performed a prospective, nonrandomized trial comparing the use of a windowed TCC to that of an offloading shoe. Patients with moderate and severe PAD were included in the study. Moderate PAD was defined as presence of at least 1 nonpalpable pedal pulse with arterial lesion detected by Doppler ultrasound and maintenance of at least 1 major artery to the foot, a TCOM between 20 mm Hg to 30 mm Hg, a history of successful revascularization and no ischemic trophic disorders, and no necrosis or gangrene. Severe PAD was defined as CLI, a wound with gangrene or necrosis, a TCOM < 20 mm Hg, failure to detect a single major artery to the foot on Doppler ultrasound, or severe arterial lesions seen on arteriography. No significant difference in age, gender, type of diabetes, duration of diabetes, body mass index, HbA1c, or ulcer duration existed between the 2 study groups. The TCC group had an increased healing rate with a decreased time to healing compared with the offloading shoe group (81% vs. 70% and 2.3 ± 1.2 months vs. 4.5 ± 4.4 months, respectively) despite the TCC group having significantly more patients with ulcerations of longer duration, greater width and depth, and midfoot Charcot foot deformity. Patient age and TCC use were the only 2 variables found to have a statistically significant positive prognostic factor for healing. The retrospective review performed herein also noted an association between TCC discontinuation and longer healing times and amputation.
Limitations
Limitations of this study include the small sample size, the paucity of literature regarding TCC use in patients with PAD, and the potential for inconclusive noninvasive vascular study results secondary to medial calcinosis and collateralization. However, given the vast variation in PAD severity and the increasing prevalence of neuroischemic DFUs that require offloading to heal, it is imperative to determine a cutoff value and definition of ischemia which absolutely precludes TCC use.
A systematic review38 of the ability of prognostic markers to predict wound healing and amputation in patients with DFUs found that a systolic ankle pressure > 70 mm Hg or the combination of a systolic ankle pressure > 50 mm Hg with an ABI > 0.5 was found to have the largest positive likelihood ratio for prediction of amputation, independent of the wound care and offloading modalities employed. Similar results and recommendations were found in the present retrospective case series and systematic review. While ABI results in patients with diabetes have been reported to be falsely elevated half the time, an ABI is still the most common noninvasive vascular study performed to determine adequacy of arterial supply. When the results are unobtainable or inconclusive, further studies that have been shown to be less likely to be affected by medial calcinosis and collateralization such as a TBI or TCOM have been employed.39,40 Thus, cutoff values for systolic ankle and toe pressure and TBI also were determined for this study. Formal vascular evaluation should be obtained for any patient in which the concern for PAD exists. Providers also must perform individual patient risk and benefit assessment, have staff trained in proper TCC application and removal techniques, have the ability to perform weekly and more urgent follow up as needed, and perform repetitive patient education on cast safety and maintenance to minimize potential complications in these patients.
Conclusions
Dr. Brand stated, “Only a small percentage of diabetic patients have vascular compromise to such an extent as to prevent a plantar foot ulcer from healing after the pressure of walking has been relieved.”32 He reported not having seen any lower extremity ischemia in patients with diabetes severe enough to prevent TCC use during 17 years of practice.32
This retrospective case review and systematic literature review to include data from other studies on TCC use in patients with PAD suggest that TCC use in patients with an ankle pressure ≥ 80 mm Hg, a toe pressure ≥ 74 mm Hg, an ABI ≥ 0.55, or a TBI ≥ 0.55 may be a viable treatment option for pressure-related neuropathic ulcerations. Discontinuation of TCC was associated with longer healing times and amputation. Vascular evaluation should be employed in all patients with PAD and a pressure-related neuropathic ulceration. Repeat evaluation should be obtained if the wound fails to progress towards resolution with TCC use.
Acknowledgments
Affiliations: Limb Salvage & Amputation Prevention Services, Restorix Health Wound Healing Center of Saint Vincent Hospital, Worchester, MA; Program Director, Restorix Health Wound Healing Center of Saint Vincent Hospital; Medical Director, Great River Wound and Hyperbaric Medicine Clinic, West Burlington, IA; and Scriptum Medica Medical Writing, University Place, WA
Correspondence: Valerie Marmolejo, DPM, Medical Writer, Scriptum Medica Medical Writing, P.O. Box 65965, University Place, WA 98466;
www.scriptummedica.com; vlsdpm@gmail.com
Disclosure: The authors disclose no financial or other conflicts of interest. The opinions or assertions contained herein are the private view of the authors and are not to be construed as official or reflecting the views of Saint Vincent Hospital.
References


Current Issue
Sign Up Today





{kind=link}
{kind=link}
{kind=link}
{kind=link}
